Real-time, accurate cardiac arrest documentation benefits everyone involved
When a patient suffers cardiac arrest in the hospital, it is terrifying for family members to witness as a loved one’s heart stops. Any family members present are ushered out of the room while the code blue team rushes in to do their jobs. The emergency response looks and feels like chaos, and it may not play out like it does on television.
As the code team fights to save a patient’s life, one team member is charged with keeping time and documenting every action taken. Often the code recorder scribbles notes on paper or any nearby surface. They don’t have time to worry about neatness.
However, when the code is over, it’s critical that the report is transcribed into the hospital EMR so it is part of the patient’s record. If the handwriting is illegible, or the notes are misplaced, the facts related to the in-hospital cardiac arrest (IHCA) may be incomplete or inaccurate.
A freestanding IHCA clinical document was absent in 50 of 101 (50%) patients.
Source: Resuscitation Journal, March 2017
In cases where the patient survives, the code blue documentation gives doctors and nurses in the ICU valuable information to continue the patient’s care.
If the patient does not survive, the doctor may use the code blue report to explain what happened to the family. The hospital may examine the notes to understand why the patient died and to evaluate the care given. The documentation also may be used as evidence in a medical malpractice lawsuit.
Documentation influences perception of care
Lawrence Logback of the law firm Simpson, Logback, Lynch, Norris, P.A. is a defense attorney who handles primarily medical malpractice lawsuits, representing hospitals and doctors. Logback said he often references code blue documentation as he prepares a case.
“Most of the time it is a scanned PDF of handwritten notes,” Logback said. “Sometimes there are handwritten notes and typed notes in the EMR that have been transcribed after the code. Often these two accounts do not match. There may have been different people recording during the code, different thought processes, looking at different clocks or watches – all of this leaves room for inconsistencies.”
Logback described how the family’s experience in the hospital, and their perceptions of the care their loved one received, can influence what happens next.
“If you have hand-scribbled notes that are not organized or don’t capture everything, that doesn’t communicate a sense of confidence to the family.”
— Lawrence Logback, Attorney

The family’s perception of the care team – either “they did everything they could” or “they didn’t know what they were doing” – can influence whether or not a lawsuit is filed.
Logback explained the immediate benefits of having timely, accurate documentation.
“If the documentation is understandable, the staff can tell the family, ‘Here’s what we did and why, we did everything we could,’ and the family can follow and understand it, that goes a long way,” he said. “Sometimes the issue for the family is ‘we don’t want this to happen to anyone else’ and having accurate documentation can lead the hospital to more training and better ways of doing things,” Logback explained.
Technology enables better code blue documentation
Documenting a code with handwritten notes on paper is error prone and archaic. Electronic documentation tools within some hospital EMR/EHR systems do exist, but often they are cumbersome, without an intuitive user interface. They are built to be used at a desktop computer, not at the patient’s bedside.
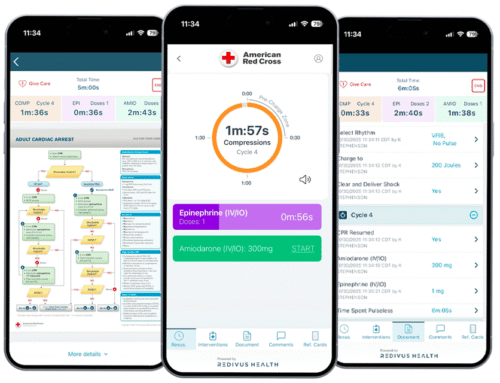
Today’s mobile technology enables easier, more accurate ways to document a code. For instance, the Redivus Code Blue app provides guided, digital documentation during a cardiac arrest from a phone or tablet. Any member of the code team can start the Redivus app and use it to keep time, record compressions and medications, and document every intervention.
At the end of the code, the Redivus solution delivers time-stamped, detailed documentation. This report can be sent to the hospital EMR and signed electronically by the physician who led the code.
“Each code event is individualized, but with the standardized documentation from Redivus, it’s happening in real time versus what I scratched on a piece of paper and then went back to enter later. Or where my adrenaline is so overloaded, I only caught half of it and then I’m going to document half of that, so I’m getting one fourth of what happened.”
“As a code documenter, you may be coming in a minute or two after the event started, but with Redivus you can go back and put in those things that happened before you arrived. You get a pretty accurate picture of what happened with the accurate times. As far as documentation, it’s a huge win.”
— Liz Doll, Clinical Nurse Leader, USA Health University Hospital
Redivus resuscitation app captures more data
Redivus Health worked with a large hospital client to perform side-by-side comparisons of data from their EHR documentation system with the Redivus data. This comparison revealed that the Redivus software collected, on average, 3x more data points than the hospital EHR, providing more complete and accurate documentation of each cardiac arrest.

All of that Redivus code data can be easily aggregated, stored and accessed in the EHR for continued patient treatment and hospital reporting within minutes of the code ending.
Why leave something so important to chance?
Medical malpractice lawsuits will always be an issue for hospitals. Having more accurate code blue documentation gives hospitals and staff the confidence to know their data is correct, organized and easily accessible when needed.
Making a switch to digital documentation yields additional benefits in terms of staff morale, team communication, quality of patient care, workflow efficiencies, and clinical insights.
“You can have perfect documentation and still have a bad outcome. Not everyone can be saved,” Logback said. “As lawyers, we recognize the value of accurate documentation and know that documentation as it stands today is a problem. The Redivus Code Blue app could help protect hospitals from unnecessary litigation.”
— Lawrence Logback, Attorney
Learn more about the Redivus app for resuscitation and cardiac arrest documentation. Request a demo to see how it works.